A special thank you to Judy Tran for developing this amazing case report.
Introduction:
The prevalence of keratoconus (KCN) in the United States is approximately 8.8-229 per 100,000 affecting both men and women equally.1 KCN is a progressive disease resulting in ectasia of the corneal stroma. It is a noninflammatory process that causes a decrease in patient visual acuity (VA) from the changes in corneal shape that leads to an increase in myopia and irregular astigmatism. What causes KCN is still not completely understood but there are studies that show a correlation between the disease and environmental factors such as eye rubbing, a family history of the disease, and atopy. Age, ethnicity, contact lens use, as well as exposure to sunlight are also observed environmental risk factors for KCN. Genetically, there has been some evidence of genes VXX1 and SOD1 being highly associated with the pathogenesis of the condition which is autosomal dominant but can occur in a sporadic pattern.2
There is currently no cure for KCN, however corneal collagen cross-linking (CXL) has been shown to have promising results in slowing the progression of the disease especially in cases involving severe progressive KCN. CXL utilizes riboflavin and a photo-oxidative reaction to increase corneal stiffness by altering the collagen within the corneal tissue. The changes to the collagen consist of increasing the number of covalent bonds and increasing the resistance to enzymatic degradation.3 CXL has been widely used in many countries for managing KCN, but it was only just recently FDA approved in the United States April 2016 and this method of treatment is becoming increasingly popular since its approval. Before the development of CXL, a corneal transplant was the only treatment for KCN but is indicated only when the disease had progressed into more advanced stages. Even after a corneal transplant, patients are still at risk for developing KCN again in the transplanted cornea. Another major complication post corneal transplant is glaucoma. There is a significant risk for the development of glaucoma after a corneal transplant as seen in a study conducted by Zheng et al.4 Depending on the severity of glaucoma, treatment could be lifetime eye drops or even requiring another ocular surgery. Just like KCN, glaucoma is an uncurable condition that can lead to blindness. Even though CXL and corneal transplant are both FDA approved methods for treating KCN, they do not always help with the major side effect of the disease which is reduced vision.
Due to the optics of an irregular cornea often seen in KCN, spectacles often cannot correct the vision. Specialty contact lenses are typically used to help maximize vision. Usually, a corneal rigid gas permeable contact lenses (RGPCL) are often indicated initially but with recent advancements, scleral rigid gas permeable contact lenses (ScCL) have shown to be an excellent, safe, and effective alternative.5 Since the scleral contact lenses do not interact with the cornea, there is a therapeutic benefit to using the larger lens especially in patients with severe dry eye. There is a liquid layer between the ScCL and the cornea which can provide constant hydration to the corneal cells. ScCL are often reserved for more severe KCN but with their material and fitting advancements, it should be an option at any stage of the condition to help patients achieve their best potential VA as well as to delay the possible need for a corneal transplant.6 This case report supports the benefits of using a ScCL for a patient with a moderate and severe KCN. By using a more custom fitted ScCL, the patient was able to reach a VA of 20/20 with optimal comfort and the ScCL could potentially reduce their need for a corneal transplant later in life.
Case description:
Visit 1: The consultation. Patient DB, a 51-year-old Hispanic male, was referred to the Contact Lens Institute of Nevada after completing a comprehensive eye exam at a Sam’s Club Optical in May 2021. The referring optometrist diagnosed the patient with myopia, astigmatism, and bilateral keratoconus with the right eye being more severe than the left. There was no spectacle prescription recommended at this time due to the severity of the KCN. The patient was advised that a specialty contact lens would provide better vision than glasses.
DB’s medical history was unremarkable, the patient had denied any medical diagnosis, medications, and allergies. The patient was unaware of any KCN prior to the eye examination in May 2021. The patient had also denied any other ocular conditions and surgeries.
Entering unaided VA were OD 20/200 and OS 20/25. Anterior segment evaluation revealed corneal central inferior thinning with striae OU. Corneal thinning and striae were mild in OS and significantly worse in OD. Fluorescein dye evaluation revealed mild SPK staining over the cone apex of OD. There were nasal and temporal pingueculas noted OU. The rest of the anterior segment was unremarkable. Posterior health was evaluated via retinal imaging which was unremarkable. There were no signs of glaucoma, macular degeneration, or any retinal disease that could possibly contribute to the patient’s reduced vision.
A KCN pattern was observed in the topometric exam (Figure 1). An OCT and a scleral mapping (sMAP) were performed over DB’s naked eye (Figure 2). The results of the exam are listed in Table 1. Based on the topography and scleral elevation (Figure 3), a Europa diagnostic lens was selected for both eyes and the parameters of the diagnostic lenses are seen in Table 2. The suggested lenses are based on a sagittal depth (Table 1), the sMAP software determines the sagittal depth assuming a chord length of 16mm and incorporating a 300um buffer. The lenses were allowed to settle for approximately 5 minutes before assessing the vision and fit, as well as an auto-refraction/keratometry over the diagnostic lens (Table 3). The over-refraction (Table 3) was determined with the starting point measured with the auto-refractor.
Figure 1: Using the Medmont, corneal topography reveals a KCN pattern in both OD and OS.

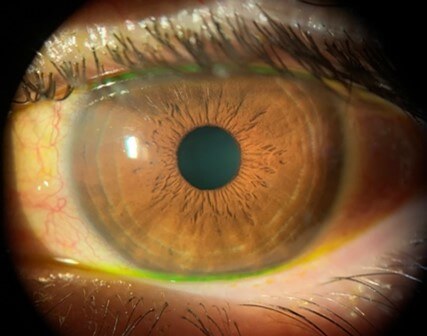
Figure 2: Images of DB’s naked eye with trace sodium fluorescence that was instilled prior. Photos were taken during the slit-lamp examination with the ION Imaging system.
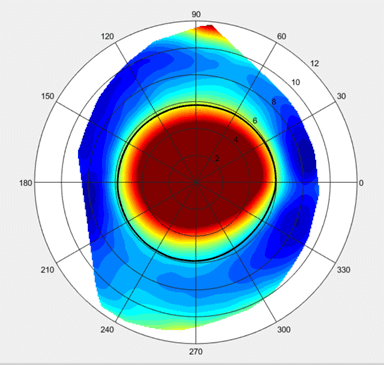

Figure 3: sMAP scleral elevation of DB’s OD and OS.
| Measurements over naked eye | OD | OS |
| Pachymetry (OCT) | 405um | 491um |
| Keratometry (Topo) | 56.43D @ 160°/ 71.61D | 43.21D @ 2°/ 46.38D |
| Corneal Cylinder (Topo) | 15.18D | 3.17D |
| Scleral Toricity (sMAP) | 214um | 270um |
| Sagittal Depth | 4479um | 4456um |
Table 1: Measurements taken over DB’s naked eyes.
| Diagnostic Lens Parameters | OD | OS |
| Base Curve | 45.00D | 46.00D |
| Sagittal Depth | 4560um | 4660um |
| Power | -1.50D | -2.00D |
| Overall Diameter | 16.0mm | 16.0mm |
| Optic Zone Diameter | 0.2mm | 0.2mm |
| Center Thickness | 0.4mm | 0.4mm |
| Material | HEXA100 | HEXA100 |
Table 2: The Europa Lens made by Visionary Optics were the diagnostic lenses used.
| Lens Assessment | OD | OS |
| Central Clearance | 58um – over apex | 388um |
| Limbal Clearance | Present 360° | Present 360° |
| Lens edges | Flat 360° | Flat 360° |
| Impingement or Blanching | Negative 360° | Negative 360° |
| Auto-refraction | +0.25 -2.50x067 | -1.50 -1.50x095 |
| Auto-keratometry | 43.50D @ 162°/ 43.75D | 43.75D @ 161°/ 44.00D |
| Over-refraction in Phoropter | -0.25 -2.50x080 | -1.00 -1.75x095 |
| VA with Over-refraction | 20/20-2 | 20/20 |
Table 3: Fit and vision assessment of the diagnostic Europa Lens on the patient’s eyes.
Due to the DB’s high scleral toricity and high internal cylinder, a custom impression ScCL was recommended for both eyes to maximally optimize visual acuity and fit but other fitting modalities were also discussed to the patient. The patient had opted for the premium custom fit for their right eye, the eye with more severe KCN and the advanced custom fit for their left eye. The premium custom fit uses an impression of the eye, similar to a dental mold, to design a lens with a 3D scanner and utilizes three million data points from the mold (Figure 4). The advanced custom fit uses the scleral mapping scan of the eye, and that special software is able to design a lens from a million data points. Two impressions of the right eye for the custom EyePrint Prosthetic were completed in-office (Figure 5) and the sMAP images that were taken were sent to the Visionary Optics Lab for the advanced custom ScCL fit for the left eye. All images and the over-refraction were sent to both labs for the lens design.

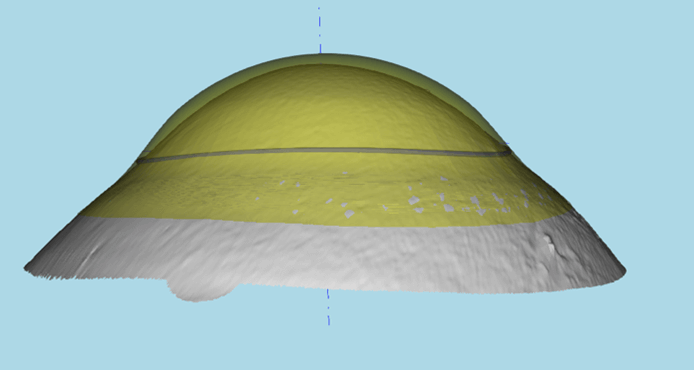
Figure 4: Front surface and back surface design of the custom EyePrint Prosthetic ScCL for DB’s right eye.

Figure 5: A visual of how the eye impression is completed for the EyePrint Prosthetic. Note: the patient in the image is not the patient in the case report.
The patient was expected to return to clinic once the ScCL arrive for a training session before being dispensed.
Visit 2: Training and dispense. An EyePrint Prosthetic ScCL was ordered for the right eye and a Latitude ScCL was ordered for the left; lens design parameters are listed in Table 4. The ScCLs were inserted for DB shortly after their arrival (Figure 6). The lens was allowed to settle for approximately 10 minutes before checking VA (Table 5) and assessing the lenses (Table 6). The clearance was determined with an anterior segment OCT (Figure 7), which was checked at the center and limbus of the cornea. Before the training session, an over-refraction was completed with the auto-refraction as the starting point and VA was measured (Table 5). Throughout the over-refraction, the patient reported fluctuating vision with may have been due to the lens settling which affected the reliability of the over-refraction.
| Lens Parameters | OD (EyePrint Prosthetic) | OS (Latitude Scleral Lens) |
| Base Curve | 8.336mm (40.49D) | 7.55mm (44.70D) |
| Sagittal Depth | 5788um | 5134um |
| Power | +2.75 – 2.38x080 | -1.67 -1.75x095 |
| Overall Diameter | 18.0mm | 16.5mm |
| Center Thickness | 0.527mm | 0.30mm |
| Material | Optimum Extra | Optimum Extra |
Table 4: Custom ScCLs parameters received by the manufactures.
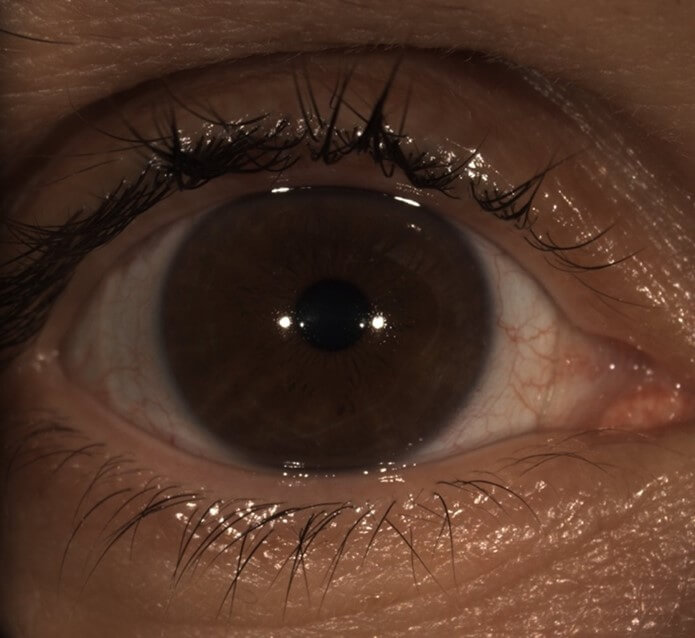

Figure 6: DB with custom EyePrint Prosthetic on OD and custom Latitude lens on OS.
| Vision Assessment | OD | OS |
| Entering VA | 20-20 | 20/50 |
| Auto-refraction | +1.50 -1.25x022 | +0.25 -1.00x136 |
| Auto-keratometry | 40.25 @ 078/ 42.00 | 41.75 @ 069/ 42.50 |
| Over-refraction in Phoropter | +0.50 -1.50x120 | +1.25 -1.50x126 |
| VA with Over-refraction | 20/25+2 | 20/20-1 |
Table 5: Vision assessment through custom ScCL.
| Lens Assessment | OD | OS |
| Centration | Centered | Centered |
| Central Clearance | 252um – over apex | 396um |
| Limbal Clearance | Acceptable 360° | Acceptable 360° |
| Lens edges | Flat 360° | Mild nasal edge lift |
| Movement | 0.25mm | 0.25mm |
| Lens Marker Location | 6:00 | 7:00 |
| Impingement or Blanching | Negative 360° | Negative 360° |
| Conjunctival Prolapse | None | 11:00 to 1:00 |
Table 6: Lens assessment of the custom ScCL on DB’s eyes after 10 minutes of settling.
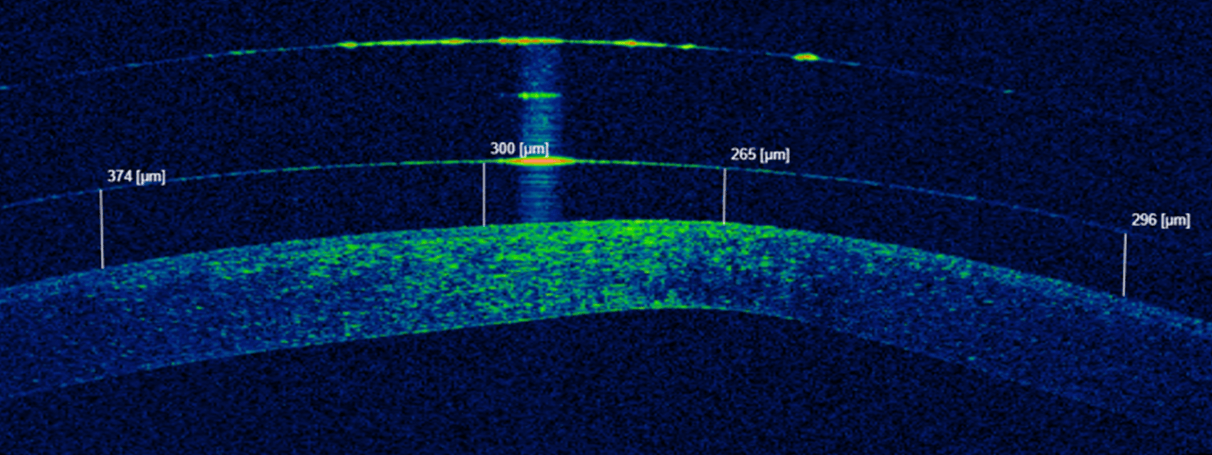

Figure 7: Anterior segment OCT reveals central clearance of the ScCL on the eyes. Top photo: OD, bottom photo: OS.
After lens evaluation, DB was educated on how to properly insert and remove the scleral lenses by using a DMV to insert and a small plunger to remove. The patient was taught how to clean and store the ScCLs using Tangible Clean Multipurpose Solution and to use sodium chloride preservative-free saline to fill the lens bowl prior to insertion. DB had no difficulties with removing the lenses with the use of the small plunger. They were advised to stick the plunger inferiorly of the lens rather than directly center, this creates an uneven pressure of release for the lens to come off the scleral resting points. There were some difficulties with insertion, DB has deeper set eyes and larger hands, so they found it difficult to maneuver the lens into the eye when they used one hand to open the upper lid and the other hand to hold the lower lid and DMV plunger with the ScCL. The technique that was most comfortable for DB was using one hand to hold the upper and lower lid while the other hand solely guided the DMV and ScCL. A scleral stand was suggested to patient which would essentially act as a third arm allowing the patient to comfortably hold open the eyelids with both hands as the move towards the scleral stand that props up the DMV and ScCL. DB expressed feeling comfortable with insertion without the need of the scleral stand. DB successfully completed training by removing and inserting the ScCL once leaving the clinic with them on, and DB was scheduled to return to the clinic in a week for a follow-up to recheck their visual acuity and the fit. The patient was advised to wear the lenses as much as possible to allow for adaptation.
Visit 3: 1 week follow-up. Case History: DB had worn the ScCL OU for 4 hours prior to the appointment. Average wear time was about 1 to 2 hours, and this was due to their eyes feeling fatigued during wear. There were difficulties with reading and intermediate distance because their eyes felt like the vision was too overwhelming which caused the eyes to feel tired. DB reports seeing better at intermediate distances without ScCL. With lenses, OD vision is much clearer than OS vision. There was mild discomfort with the OS at the appointment but denies and redness from the ScCL. The patient also noted that there were some difficulties with insertion because they could not get their eyes wide enough, but ScCL removal was easy with the use of the small plunger. The fit of the ScCL was reassessed (Figure 8), clearance was determined with the anterior segment OCT (Table 7 and Figure 9), auto-refraction/keratometry was completed, and an over-refraction was measured with the auto-refraction as a starting point (Table 8).


Figure 8: 1-week follow-up with custom ScCL with Eyeprint Prosthetic for OD and Latitude Lens for OS.
| Vision Assessment | OD | OS |
| Entering VA | 20/20-1 | 20/50 |
| Auto-refraction | +1.25 -1.00x012 | +1.25 -2.75x109 |
| Auto-keratometry | 40.25 @ 078/ 41.75 | 41.50 @ 025/115 |
| Over-refraction in Phoropter | +0.25DS | +0.75 -1.75x135 |
| VA with Over-refraction | 20/20-2 | 20/20-1 |
Table 7: Vision assessment through custom ScCL at 1 week follow-up.
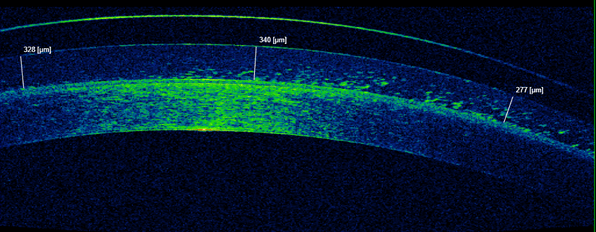
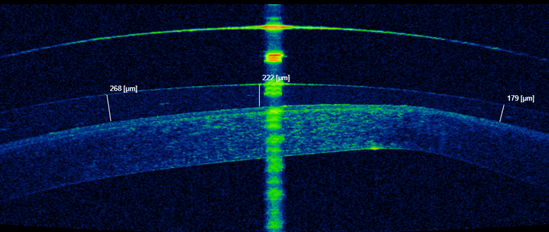
Figure 9: Anterior segment OCT after 4 hours of ScCL wear on the eyes at 1-week follow-up. Top photo: OD, bottom photo: OS.
| Lens Assessment | OD | OS |
| Centration | Centered | Centered |
| Central Clearance | 222um | 340um |
| Limbal Clearance | Acceptable 360° | Acceptable 360° |
| Lens edges | Flat 360° | Flat 360° |
| Movement | Minimal | Minimal |
| Lens Marker location | 6:00 | 8:00 |
| Impingement or Blanching | Negative 360° | Negative 360° |
Table 8: Lens assessment of custom ScCL after 4 hours of wear.
Since the patient had difficulties with near and intermediate vision, a monovision fit was discussed to maximize acuity at all distances and to improve patient visual comfort. However, with the monovision fit, it was discussed that distance vision may be reduced to compensate for near vision. It was also educated to the patient that with a monovision fit, depth perception will be reduced. A monovision fit was trial framed and DB could not adapt to the vision. The patient opted to best correct distance vision in the ScCL for part-time wear and was educated that an over-the-counter reading spectacle prescription will be necessary to optimize near vision.
The overall fit of the lenses was acceptable, the only modification needed was to change the prescription of the left eye since the patient entering visual acuity was 20/50. A new lens was ordered to adjust the lens prescription incorporating the over-refraction that was determined (Table 7). The patient will continue with the right lens to allow more time to adapt. Another modification that will be considered at the next dispense appointment is possibly making the OD ScCL a smaller diameter for easier insertion. The patient is to return to the clinic for a new OS latitude ScCL dispense when it arrives.
Discussion:
Before the development of the corneal topographer, the only way to diagnose KCN was through slit lamp observed clinical signs, therefore it was often not diagnosed until later stages. Corneal signs such as corneal protrusion, corneal apex thinning, Vogt’s striae, Fleisher’s ring, and possibly corneal scarring typically represent more advanced stages of the condition. In earlier stages of KCN, patient symptoms can include reduced vision due to an increase in myopia and irregular astigmatism, visual distortions, and light sensitivity. Because of the constant changes in vision, patients with KCN may need to frequently change their spectacle correction. Now that the corneal topographer is becoming increasing popular and more readily available, early stages of KCN can be more easily diagnosed with the technology and treatment such as CXL can be implemented sooner to slow down the disease progression, ultimately preserving the patients’ vision.1 A 10-year study conducted by Raiskup et al. showed that CXL treatment was effective in decreasing the progression of the disease as well as stabilizing the cornea long-term ultimately reducing the need for a corneal transplant. By decreasing the progression of the disease by stabilizing the cornea, vision is preserved. CXL provides treatment in early diagnoses especially in adolescents with less complications compared to a corneal transplant.7 The Nordstorm et al. study demonstrated that after a year post CXL treatment in KCN subjects had decreased corneal irregularities and improved vision. There was also no damage or any cell loss to the corneal endothelium. The study demonstrated that CXL treatment for KCN is not only effective in slowing the progression of the disease, that the procedure is also safe.8
In early stages of the disease, a spectacle correction can provide adequate vision, however as the disease progresses, glasses are unable to mask the irregular astigmatism that typically occurs. Corneal RGPCL are common for correcting keratoconus. However, ScCL are becoming increasing popular because of they provide better patient comfort compared to corneal RGPCL. In a study conducted by Levit, Benwell, and Evans, they found that although there was no significant difference in vision or vision quality of life, KCN patients preferred ScCL over corneal RGPCL because of the significant difference in comfort.9 ScCL are typically preferred over corneal RGP because of their design, they rest only on the sclera which allows the lens to vault over the cornea entirely. This minimizes any interaction between the cornea and the contact lenses. ScCL can also help reduced the need of a corneal transplant in patients with severe keratoconus, which was observed in a study by Koppen et al. A majority of subjects with severe KCN had a decreased need for a corneal transplant when they were successfully fitted with a ScCL. Subjects that underwent a corneal transplant even after a ScCL fit was due to their inability to tolerate the lens.6 By fitting KCN patients with ScCL rather than treating with a corneal transplant, this is reduced the complications associated with the surgical procedure such as glaucoma.
A retrospective study by Fuller and Wang assessed the prevalence of ScCL complications such as microbial keratitis, phlyctenulosis, cornea abrasion, contact lens-induced acute red eye, corneal infiltrates, pingueculitis, and hydrops. The complications were observed to be related to poor wetting, poor handling, reservoir fogging, lens intolerance, deposits in the eye, and broken lenses in the eye. Although the adverse effects occurred in a small percentage of subjects in the study, they can still occur with any ScCL, therefore proper ScCL fitting, and patient education is important to reduce the risk of any complications. Other management options for complications were adding a surface treatment to the lens, replacing the lens, and adjusting the wear time. Overall, the study concluded that ScCL for KCN patients are safe and effective.5
Most traditional ScCLs design assume that the sclera is a uniform, spherical shape, however, this is not the case for many individuals. With the use of a sMap3D corneo-scleral topographer, DeNaeyer et al. measured not only the elevation of the cornea, but the elevation of the sclera as well on 140 eyes. They determined that approximately only 5.7% of the eyes had a spherical scleral shape, 28.6% had a regular toricity, and actually 40.7% had asymmetric elevations and depressions. This means that a majority of the population have a non-spherical scleral yet, most practitioners continue to fit scleral lenses empirically with a traditional lens design. Common complications often seen with ScCLs that have a poor landing on the sclera is conjunctival blanching, conjunctival prolapse and can even potentially result in staining of the surface tissues.10 By determining the patient’s scleral shape at the initial visit, it can help potentially decrease fitting chair time and improve patient comfort with the ScCL.
In the case of DB, their stage of KCN was well advanced, especially in their right eye, therefore their reduced vision of 20/200 could not be corrected with glasses. Scleral lenses were selected over a corneal RGP lens for maximum comfort and optimal visual acuity. A more custom fit ScCL was chosen over a traditional fit because of the patients high scleral toricity that was determined initially at the consultation appointment. A well-fitted ScCL was achieved just after one visit and by using a more custom ScCL design, such as the Latitude and EyePrint Prosthetic ScCL, the patient was able to achieve 20/20 vision in the poorer 20/200 seeing eye while maximizing the lens comfort reducing any risk of ScCL complications. Hopefully, by fitting DB in a ScCL it reduces their need for a corneal transplant later.
Conclusion:
Fitting a ScCL can be intimating and has a poor stigma of being difficult and time consuming, requiring a lot of follow-ups and lens adjustments. However, with advancements in corneal imaging and mapping, diagnosing KCN and fitting ScCL is much simpler with less chair time. By gaining the confidence to fit ScCL, the care and services can be provided to KCN patients without the need for an additional referral. ScCL have been shown to be safe and effective for achieving optimal vision for KCN patients even after a couple of months post CXL treatment. By diagnosing KCN in earlier stages, CXL can be implemented to immediately stabilize the cornea before the disease progresses, then with the added ScCL fit, the potential need for a corneal transplant is significantly reduced along with the associated complications with the surgical procedure.
References:
- Leucci, M., & Carter, M. (2018). Clinical signs in keratoconus. Optometry Today (London), 58(11), 86.
- Hashemi, H., Heydarian, S., Hooshmand, E., Saatchi, M., Yekta, A., Aghamirsalim, M., Valadkhan, M., Mortazavi, M., Hashemi, A. & Khabazkhoob, M. (2020). The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea, 39 (2), 263-270. doi: 10.1097/ICO.0000000000002150.
- Vinciguerra, R., Romano, M. R., Camesasca, F. I., Azzolini, C., Trazza, S., Morenghi, E., & Vinciguerra, P. (2013). Corneal cross-linking as a treatment for keratoconus: Four-year morphologic and clinical outcomes with respect to patient age. Ophthalmology (Rochester, Minn.), 120(5), 908-916. https://doi.org/10.1016/j.ophtha.2012.10.023
- Zheng, C., Yu, F., Tseng, V. L., Lum, F., & Coleman, A. L. (2018). Risk of glaucoma surgery after corneal transplant surgery in medicare patients.American Journal of Ophthalmology, 192, 104-112. https://doi.org/10.1016/j.ajo.2018.05.004
- Fuller, D. G. & Wang, Y. (2020). Safety and Efficacy of Scleral Lenses for Keratoconus. Optometry and Vision Science, 97 (9), 741-748. doi: 10.1097/OPX.0000000000001578.
- Koppen, C., Kreps, E. O., Anthonissen, L., Van Hoey, M., Dhubhghaill, S. N., & Vermeulen, L. (2018). Scleral lenses reduce the need for corneal transplants in severe keratoconus.American Journal of Ophthalmology, 185, 43-47. https://doi.org/10.1016/j.ajo.2017.10.022
- Raiskup, Frederik, MD, PhD, FEBO, Theuring, A., MD, Pillunat, L. E., MD, & Spoerl, E., PhD. (2015). Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: Ten-year results.Journal of Cataract and Refractive Surgery, 41(1), 41-46. https://doi.org/10.1016/j.jcrs.2014.09.033
- Nordström, M., Schiller, M., Fredriksson, A., & Behndig, A. (2017). Refractive improvements and safety with topography-guided corneal crosslinking for keratoconus: 1-year results.British Journal of Ophthalmology, 101(7), 920-925. https://doi.org/10.1136/bjophthalmol-2016-309210
- Levit, A., Benwell, M., & Evans, B. J. W. (2020). Randomised controlled trial of corneal vs. scleral rigid gas permeable contact lenses for keratoconus and other ectatic corneal disorders.Contact Lens & Anterior Eye, 43(6), 543-552. https://doi.org/10.1016/j.clae.2019.12.007
- DeNaeyer, G., Sanders, D., van der Worp, E., Jedlicka, J., Michaud, L., & Morrison, S. (2017). Qualitative Assessment of Scleral Shape Patterns Using a New Wide Field Ocular Surface Elevation Topographer: The SSSG Study. Journal of Contact Lens Research and Science, 1(1), 12-22. https://doi.org/10.22374/jclrs.v1i1.11
